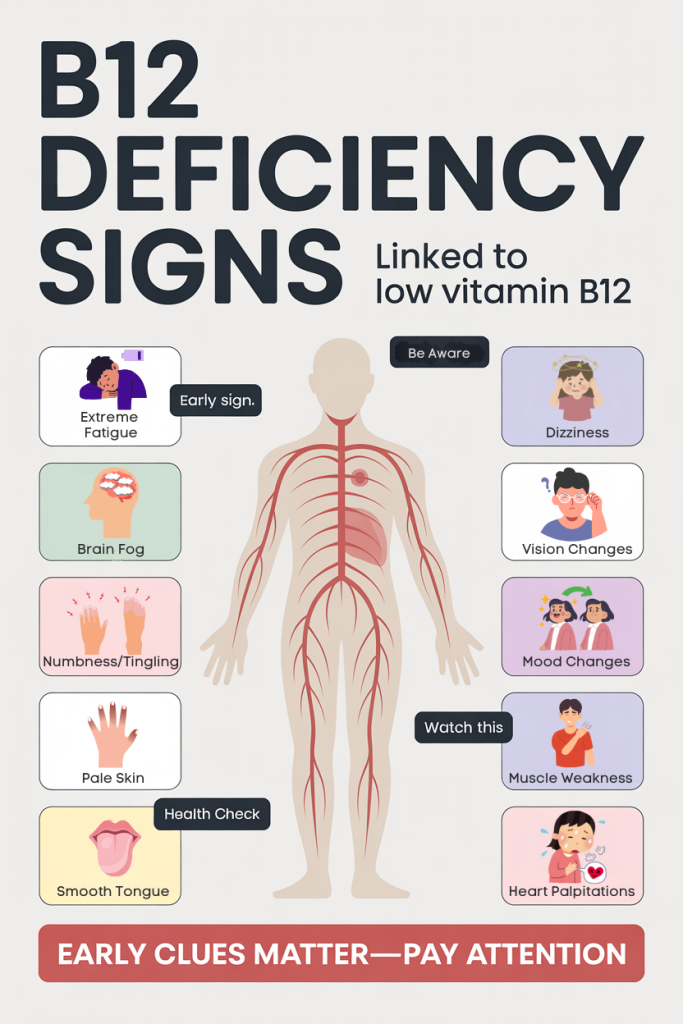
10 Warning Signs Of Vitamin B12 Deficiency You Shouldn’t Ignore — How To Spot Symptoms Early
Vitamin B12 deficiency is far more common than most people realize, and yet it often hides behind vague symptoms that we dismiss as stress or aging. In 2026, with more people following plant-based diets, living longer, and taking medications that affect absorption, recognizing early signs of low B12 is essential. In this text we’ll walk through the top ten warning signs of vitamin B12 deficiency, why the vitamin matters for brain, blood, and energy, who’s most at risk, and how spotting symptoms early can prevent long-term damage.
We’ll use clear, evidence-based explanations and practical red flags you can watch for, so you and your healthcare provider can act before problems become severe. If you’ve been feeling off, fatigued, forgetful, numb, or unusually moody, there’s a realistic chance vitamin B12 is part of the picture. Read on to learn what to look for and what steps we recommend taking if you suspect deficiency.
Why Vitamin B12 Matters For Your Brain, Blood, And Energy
Vitamin B12 (cobalamin) is one of the B vitamins that keeps our nervous system, red blood cell formation, and cellular energy production running smoothly. At a biochemical level, B12 acts as a cofactor for enzymes involved in DNA synthesis and the metabolism of fatty acids and amino acids. Two pathways are particularly important: methylation of homocysteine to methionine (affecting brain function and cardiovascular risk) and conversion of methylmalonyl-CoA to succinyl-CoA (affecting nerve health). When B12 levels fall, these pathways slow, and we start to notice symptoms.
For the brain, inadequate B12 can impair neurotransmitter synthesis and myelin maintenance, the insulating sheath around nerves, leading to cognitive and sensory problems. In the blood, B12 deficiency disrupts red blood cell maturation, causing megaloblastic anemia: red cells are fewer, larger, and less efficient at carrying oxygen: that’s why fatigue and pale skin are common complaints. Energy levels drop as mitochondrial function and cellular metabolism degrade.
Beyond these core roles, B12 interacts with folate and vitamin D status and may influence mood and sleep. Because the signs can be subtle and overlap with other conditions (thyroid disease, depression, aging), we need to keep B12 on our diagnostic radar. Early detection is crucial: neurological changes may be partially reversible if treated promptly but can become permanent if overlooked.
Who Is Most At Risk And Why Early Detection Helps
Certain groups face higher risk for vitamin B12 deficiency, and understanding who they are helps us prioritize screening and early action. First, older adults: stomach acid and intrinsic factor decline with age, reducing B12 absorption from food. Studies show B12 deficiency rates rise significantly after age 60. Second, people following strict vegan or long-term vegetarian diets are at risk because B12 is naturally found primarily in animal-derived foods, although fortified foods and reliable supplements work well.
Third, individuals with gastrointestinal disorders or surgical histories, Crohn’s disease, celiac disease, small intestinal bacterial overgrowth (SIBO), or resection of the ileum or stomach, often have impaired absorption. Fourth, people taking certain medications long-term, metformin for diabetes and proton pump inhibitors/H2 blockers for reflux, can develop low B12. Finally, pernicious anemia, an autoimmune condition that destroys intrinsic factor, is a classic cause and requires specific treatment.
Early detection matters because some effects, especially neurological damage and peripheral neuropathy, can become permanent if deficiency persists. Treating B12 deficiency is usually straightforward, dietary changes, oral supplementation, or injections, but timing influences recovery. We recommend that at-risk individuals and anyone with suspicious symptoms get their B12 status checked (serum B12, methylmalonic acid when needed) rather than waiting until problems worsen.
Neurological And Cognitive Warning Signs
When vitamin B12 is low, cognitive and neurological systems often show the earliest, and sometimes most concerning, changes. We should be alert to progressive memory problems, slowed thinking, difficulty concentrating, and a general decline in executive function. Patients sometimes describe subtle changes at first: losing track of conversations, forgetting appointments, or needing more effort to complete complex tasks. These symptoms can mimic early dementia, so we must include B12 testing in any workup for cognitive decline.
On the neurological side, B12 deficiency can impair myelin maintenance. That leads to slowed nerve conduction and symptoms like sensory disturbances, reduced reflexes, and even changes in gait (we’ll discuss gait separately). Mood and sleep disturbances often overlap with cognitive complaints, disrupted sleep reduces cognitive reserve and can amplify perceived memory problems.
Objective testing may show slowed processing on neuropsychological tests, but labs are equally important. Serum B12 can be misleadingly normal in some people: when cognitive symptoms are present even though borderline B12 levels, methylmalonic acid (MMA) and homocysteine measurements help confirm functional deficiency. Importantly, earlier treatment correlates with better cognitive recovery, delays increase the risk of lasting deficits, so when we see persistent cognitive changes, we act quickly.
Numbness, Tingling, And Peripheral Neuropathy
One of the hallmark neurological signs of vitamin B12 deficiency is peripheral neuropathy, typically presenting as numbness, tingling, or a “pins and needles” feeling in the hands and feet. These paresthesias often start distally (toes and fingertips) and may progress over weeks to months. Many people describe it as walking on cotton or a loss of sensation that makes tasks like buttoning a shirt or picking up small objects harder.
If untreated, the sensory loss can become more pronounced and spread proximally. We may also notice decreased vibration and proprioception (sense of limb position), which worsens risk of injuries because patients don’t feel small cuts or temperature differences. Less commonly, neuropathy can manifest as burning pain or electrical shocks, symptoms that are often misattributed to diabetes or mechanical nerve compression.
Electrophysiological testing (nerve conduction studies) can confirm neuropathy, but clinical examination is usually enough to raise suspicion. Because peripheral nerve damage can be partly irreversible if longstanding, we emphasize early evaluation and treatment. When B12 deficiency is corrected, through supplementation or injections, many patients experience gradual improvement in numbness and tingling, especially if therapy begins before nerve degeneration becomes severe.
Balance Problems, Gait Changes, And Coordination Loss
Balance difficulties and changes in gait are common but underrecognized signs of B12 deficiency. When the spinal cord’s posterior columns are affected (a condition called subacute combined degeneration), our ability to sense vibration and position is impaired, and coordination suffers. Patients often report clumsiness, frequent stumbling, or a sensation of unsteadiness, especially in low light or when walking on uneven surfaces.
The gait may become broad-based and unsteady, with an increased risk of falls. Fine motor skills, like writing, buttoning, or using utensils, can also be compromised. Unlike simple muscle weakness, these problems stem from sensory impairment and disrupted proprioceptive feedback. In clinic, we’ll notice a positive Romberg sign (increased sway with eyes closed) and impaired heel-to-toe walk.
These motor and coordination symptoms are not only disabling but potentially dangerous: falls in older adults can lead to fractures and loss of independence. Fortunately, earlier intervention with B12 replacement can halt progression and often improves balance and coordination. But when spinal cord changes have been present for a long time, recovery may be incomplete, yet another reason to screen and treat promptly when we see unexplained balance or gait problems.
Fatigue, Pale Skin, And Anemia-Related Symptoms
One of the most classic clusters of vitamin B12 deficiency signs relates to anemia. Because B12 is essential for DNA synthesis during red blood cell production, low levels lead to megaloblastic anemia: red blood cells are fewer, larger, and less efficient at oxygen delivery. Clinically, we frequently see persistent fatigue, decreased stamina, and a sense of heaviness or exhaustion that doesn’t improve with sleep.
Pale skin and pallor of the nail beds are common physical exam findings. Other anemia-related symptoms include reduced exercise tolerance and lightheadedness when standing up quickly. When anemia is moderate to severe, people may notice cold intolerance and slower recovery from exertion. Laboratory tests typically show elevated mean corpuscular volume (MCV) and low hemoglobin, but mixed nutritional deficiencies (iron, folate) can mask the typical macrocytosis.
Treating B12 deficiency often leads to rapid improvement in energy and hemoglobin within weeks, though full restoration of normal red cell indices can take months. We should remember that fatigue is non-specific: checking B12 is a straightforward step when we encounter unexplained, persistent tiredness, especially if accompanied by pallor, breathlessness, or other neurologic signs.
Shortness Of Breath, Heart Palpitations, And Low Energy
Expanding on anemia-related symptoms: low oxygen-carrying capacity leads to shortness of breath with minimal exertion and palpitations or a racing heart as the body compensates for reduced oxygen delivery. These symptoms can be alarming and are frequently mistaken for primary cardiac or respiratory disease.
In practice, we evaluate vitals and look for tachycardia, low oxygen saturation (rare from anemia alone), and signs of high-output states. Orthostatic symptoms, lightheadedness or near-fainting on standing, may occur if anemia is significant. Importantly, once B12 replacement begins, many people report a noticeable improvement in breathlessness and palpitations within days to weeks as hemoglobin starts to recover.
Because cardiac symptoms may overlap with dangerous conditions, we always rule out acute cardiopulmonary causes. But in the absence of such findings, recognizing anemia from B12 deficiency saves unnecessary testing and leads to a simple corrective pathway: confirm labs, address cause (diet, absorption, medications), and start replacement.
Mood, Memory, And Sleep Changes
Vitamin B12 plays a role in neurotransmitter metabolism and methylation processes that affect mood regulation and sleep architecture. Low B12 can present as mood swings, increased irritability, anxiety, and, in many cases, depressive symptoms. Memory complaints and difficulty forming new memories often coexist, creating a feedback loop where poor sleep worsens mood and cognitive performance.
We should consider B12 deficiency in patients with new or worsening depression, particularly when antidepressants yield suboptimal results or when cognitive slowing accompanies mood changes. Sleep disturbances can include insomnia or fragmented sleep: disrupted sleep then amplifies daytime cognitive fog and emotional reactivity.
Screening for B12 in mood and sleep disorders is inexpensive and frequently informative. For patients with borderline B12 levels, we often check methylmalonic acid or use a trial of supplementation under medical supervision. While supplementation is not a replacement for comprehensive mental health care, correcting an underlying B12 deficiency can significantly improve mood, sleep quality, and cognitive resilience, and may enhance response to other therapies.
Depression, Irritability, And Brain Fog
More specifically, the triad of depression, irritability, and brain fog is a common presentation of low B12 that patients and clinicians sometimes overlook. Brain fog refers to a subjective sense of slowed thinking, difficulty concentrating, and an inability to multitask, symptoms that impact work performance and daily life. Irritability may show up as low frustration tolerance and interpersonal strain.
The link between B12 and mood is supported by biological plausibility: disrupted methylation affects serotonin and dopamine pathways. Clinical studies show higher rates of depressive symptoms in individuals with low B12, though the relationship is complex and bidirectional. Importantly, treating B12 deficiency can produce meaningful improvements in mood and clarity, particularly when deficiency is a contributor rather than the sole cause.
We recommend a practical approach: when patients present with this combination of symptoms, include B12 testing in the initial workup, consider coexisting conditions (thyroid, vitamin D, sleep apnea), and, when indicated, initiate appropriate B12 replacement while following mood symptoms closely.
Oral And Gastrointestinal Signs: Glossitis, Appetite Loss, And Digestive Changes
Vitamin B12 deficiency often shows up in the mouth and digestive tract. Glossitis, an inflamed, smooth, sore tongue, is a distinctive and visible sign. Patients describe a bright red or beefy tongue with burning pain and difficulty chewing or swallowing. Mouth ulcers, a metallic taste, and increased sensitivity to spicy foods can also occur.
Gastrointestinal symptoms extend beyond the mouth. Appetite loss, unintentional weight loss, nausea, constipation, diarrhea, and general digestive discomfort can accompany deficiency. Because B12 absorption depends on gastric acid and intrinsic factor, disorders that impair stomach function (atrophic gastritis, chronic H. pylori infection) frequently co-occur with oral and GI signs.
From a diagnostic standpoint, when we observe glossitis or new digestive complaints, especially along with neurological or systemic symptoms, we prioritize B12 testing. Treatment often relieves oral soreness quickly and improves appetite. For patients with malabsorption, addressing the underlying GI condition and using appropriate B12 routes (high-dose oral or intramuscular injections) ensures better outcomes.
Conclusion
Vitamin B12 deficiency can present in many ways, cognitive decline, numbness and neuropathy, balance problems, anemia-related fatigue, mood changes, and oral or GI signs. Because symptoms overlap with other common conditions, we need a low threshold to test at-risk patients and anyone with unexplained neurological or systemic complaints. Early detection and timely replacement (dietary counseling, oral supplements, or injections) typically lead to substantial improvement and can prevent irreversible damage.
If you recognize one or more of the warning signs described here, discuss testing with your healthcare provider: a serum B12 plus reflexive methylmalonic acid or homocysteine when indicated will clarify diagnosis. For those at higher risk, older adults, vegans, people with GI disease, or those on long-term metformin or PPIs, regular screening makes sense. Acting early preserves function, energy, and quality of life, so let’s pay attention to these signs and get ahead of deficiency.