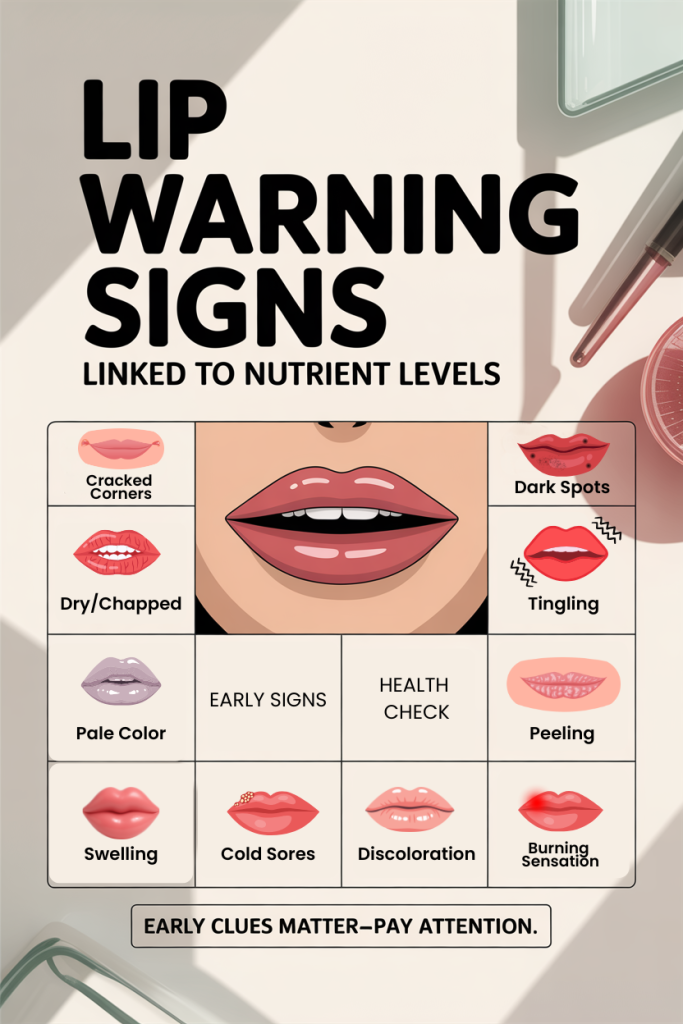
10 Lip Clues That Reveal Hidden Nutrient Deficiencies (And What To Do About Them)
Our lips are more than a smile accessory, they’re a visible, often overlooked window into our nutritional status. Over time we’ve learned to read subtle cues on the face and body, and the lips offer some of the clearest, earliest signs that something in our diet or absorption may be off. In this text we’ll walk through 10 specific lip findings, from pallor and peeling to burning and hyperpigmentation, explain the most likely nutrient connections, and give practical, evidence-based steps to test, treat, or rule out causes. We’ll focus on common, reversible deficiencies (iron, B‑vitamins, zinc, essential fatty acids, vitamin A, and more) while pointing out when a sign suggests a medical emergency or referral. Use this as a pragmatic guide: notice a change in your lips, and you’ll know which nutrients to consider, what simple dietary tweaks can help, and when to seek professional testing.
How Lips Reflect Nutrition: What To Look For And Why It Matters
Lips are thin, highly vascularized tissue with a delicate mucocutaneous junction, that combination makes them very responsive to changes in blood, hydration, and cellular turnover. When nutrient supply, absorption, or utilization is suboptimal, the lips often show early, visible changes because:
- Blood flow and oxygenation affect lip color quickly.
- The lip’s outer layer depends on healthy epithelial turnover, a process that needs vitamins, minerals, and fats.
- Immune‑related nutrients influence how well the lips handle viral, fungal, or inflammatory triggers.
What to watch for: color shifts (pale, blue, yellow), texture changes (dry, cracked, peeling, swollen), localized lesions (cold sores, angular fissures), and sensory symptoms (burning, numbness). Each sign points toward a short list of likely nutritional or physiological causes. We’ll avoid alarmist interpretations, many cosmetic or environmental causes (sun, cold, cosmetics) can mimic nutrient problems, but we’ll also highlight when a finding warrants laboratory evaluation (for example, suspected iron deficiency anemia or B12 deficiency).
Our goal is practical: when you notice a change in your lips, we’ll tell you which nutrients to consider, short-term self-care to relieve symptoms, and the objective tests or specialist referrals that clarify the diagnosis.
Pale Or Chalky Lips: Signs Of Iron Or Vitamin B12 Low Levels
Pale lips, a washed‑out pink or chalky white appearance, frequently hint at reduced hemoglobin or red blood cell mass. The two most common nutritional culprits here are iron deficiency and vitamin B12 insufficiency, both of which impair normal red blood cell formation.
Why it happens: Hemoglobin gives circulating blood its color. When hemoglobin drops (iron deficiency anemia) or when red blood cell production is ineffective (B12 deficiency, causing megaloblastic anemia), mucosal surfaces like the lips can lose their normal rosy hue.
What we typically see: uniform pale lips, often accompanied by fatigue, lightheadedness, shortness of breath on exertion, or brittle nails. With B12 deficiency you might also see glossitis (smooth, sore tongue) and neurological symptoms like numbness or balance problems.
What to do now: First, check for obvious causes, heavy menstrual bleeding, recent gastrointestinal symptoms, restrictive diets (vegetarian/vegan without B12 supplementation) or long‑term antacid use that impairs absorption. For testing, a complete blood count (CBC) with mean corpuscular volume (MCV), ferritin, serum iron, TIBC (total iron‑binding capacity), and serum B12 are appropriate initial labs.
Nutrition fixes: For iron deficiency, dietary steps include focusing on heme iron sources (lean red meat, poultry, fish) and pairing plant iron (lentils, spinach, legumes) with vitamin C to boost absorption. If ferritin is very low, oral iron supplementation (ferrous sulfate, gluconate, or fumarate) under medical guidance is standard, sometimes with gastrointestinal side effect mitigation strategies (lower dose more frequently, take with vitamin C). For B12 deficiency we recommend cyanocobalamin or methylcobalamin supplementation, the route (oral vs intramuscular) depends on the cause (dietary vs malabsorption).
When to refer: Pronounced pallor with symptoms of anemia or abnormal lab results should prompt follow‑up with a primary care provider or hematology if the cause isn’t clear. We shouldn’t ignore pale lips, untreated deficiencies can have systemic consequences.
Blue Or Purple Lips: When Oxygenation And Iron Are At Risk
Blue or purple lips (cyanosis) signal poor oxygen delivery or altered hemoglobin chemistry. While cold exposure or vasoconstriction can cause transient blueness, persistent discoloration raises concerns that require prompt attention.
Nutritional or metabolic contributors: Severe anemia can reduce oxygen content in blood and give a bluer cast to mucosal surfaces. Methemoglobinemia, a condition where hemoglobin is oxidized and can’t carry oxygen effectively, can also produce central cyanosis: it’s sometimes associated with exposure to certain oxidizing drugs or nitrates, and rare inherited enzyme defects. Certain nutritional deficiencies that severely impair hemoglobin production (advanced iron or B‑vitamin deficiencies) can be part of the picture.
Clinical context matters: Distinguish peripheral issues (cold, poor circulation, Raynaud phenomenon) from central hypoxemia (lung disease, congenital heart disease, high‑altitude exposure). If blue lips are accompanied by breathlessness, chest pain, confusion, or fainting, we treat this as a medical emergency.
Testing and action: Pulse oximetry, arterial blood gas, CBC, and methemoglobin level (if exposure risk exists) are useful immediate tests. For suspected nutrient‑related causes we still test ferritin, B12, and folate. Treatment might include oxygen, removal of the offending agent, methylene blue for methemoglobinemia in appropriate cases, and targeted repletion of any identified deficiencies.
Prevention and dietary notes: Preventing severe anemia through routine screening (especially in high‑risk groups like pregnant people, young children, and those with chronic disease) is key. Nutritionally, ensuring adequate iron and B‑vitamin intake and addressing absorption issues stops the problem before it affects oxygenation.
Yellowish Or Orange Tint: Liver Issues, Too Much Beta‑Carotene, Or Fat‑Soluble Vitamin Imbalance
A yellowish or orange tint to the lips is less common than other color changes but can point to distinct causes. We separate systemic jaundice from dietary pigment deposition and from fat‑soluble vitamin imbalances.
Jaundice and liver function: When bilirubin accumulates due to liver dysfunction, bile duct obstruction, or hemolysis, it colors skin and mucosa yellow. If lips appear yellow and the sclera (white of eyes) is also yellow, this strongly suggests hyperbilirubinemia, get liver function tests (ALT, AST, alkaline phosphatase, bilirubin fractions) and a clinical evaluation.
Dietary pigments: Eating very large amounts of beta‑carotene–rich foods (carrots, sweet potatoes, pumpkin) can cause carotenemia, which tints skin and sometimes the palmar surfaces and lips orange-yellow without affecting the sclera. It’s benign and reverses when intake normalizes.
Fat‑soluble vitamin imbalance: Excessive supplementation with preformed vitamin A (retinol) can cause skin and mucosal changes and systemic symptoms. Chronic hypervitaminosis A is uncommon but possible with high-dose supplements.
What we recommend: If the yellow tint is accompanied by fatigue, dark urine, abdominal pain, or clay-colored stools, prioritize liver testing. If the change followed a diet high in orange vegetables or heavy supplement use, try reducing intake/supplements and reassessing in a few weeks. When in doubt, ask your clinician for liver panels and a medication/supplement review before assuming a benign cause.
Dry, Cracked, Or Peeling Lips: Essential Fatty Acids, Vitamin A, And Hydration Shortfalls
Dry, chapped, or peeling lips are extremely common and often blamed on the weather, but nutritional contributors matter, especially when symptoms are persistent or severe.
Essential fatty acids (EFAs): The lipid barrier of the skin and mucosa depends on adequate omega‑6 and omega‑3 fatty acids. A diet low in EFAs undermines barrier function, making lips more prone to fissuring and trans-epidermal water loss. Topical emollients help, but without dietary correction symptoms can recur. Sources: flaxseed, walnuts, chia seeds (ALA) and fatty fish like salmon and mackerel (EPA/DHA).
Vitamin A and epithelial health: Vitamin A (and its derivatives) supports epithelial cell differentiation and turnover. Both deficiency and excess can cause mucocutaneous symptoms. In low‑income settings, vitamin A deficiency classically causes xerosis (dryness), but in our contexts, suboptimal intake combined with other stressors (cold, lip‑licking) can exacerbate dryness. Conversely, chronic high intake of preformed vitamin A may cause mucocutaneous peeling and cracking.
Hydration and electrolytes: Chronic dehydration or low electrolyte status (especially in the context of diuretics, heavy sweating, or gastroenteritis) can make lips feel dry. But oral hydration alone often isn’t sufficient if barrier lipids are depleted.
Practical steps: Use fragrance-free, occlusive balms (petrolatum, lanolin alternatives) to reduce moisture loss while addressing diet. Increase EFA intake and include vitamin A–rich foods (orange vegetables, dark leafy greens) rather than relying on high‑dose retinol supplements. If lips fail to improve with these measures or if we see severe secondary infection, patch testing for contact allergy or a dermatology referral may be warranted.
Angular Cheilosis (Cracked Corners): B‑Vitamins And Iron Connections
Angular cheilosis, painful cracks at the corners of the mouth, is a frequent clinic finding with a predictable list of nutritional associations. We see it often in people with B‑vitamin deficiencies (riboflavin/B2, niacin/B3, B6, and B12) and iron deficiency, because both sets of nutrients support mucosal integrity and immune function.
Mechanisms: B‑vitamins are coenzymes in energy metabolism and cell repair: deficiency impairs epithelial turnover and increases susceptibility to secondary infection (often Candida or Staphylococcus). Iron deficiency also weakens mucosal surfaces and delays healing.
Typical presentation: Red, painful fissures at one or both mouth corners that may bleed or crust. They often worsen with saliva pooling and may recur in people who wear dentures or have poor oral fit.
Practical approach: First rule out local mechanical causes (ill-fitting dentures, drooling) and topical irritants (lip lickers’ dermatitis). For suspected nutritional causes, we recommend a short course of targeted oral supplementation while arranging labs: a CBC, ferritin, and a B‑vitamin panel (B12, folate, possibly riboflavin/niacin if available). Topical management includes protective emollients and antifungal cream if Candida is suspected.
Dietary guidance: Encourage a balanced intake of whole grains, lean meats, dairy or fortified plant milks, legumes, nuts, and leafy greens to cover B‑vitamins and iron. If someone follows a restrictive diet (e.g., vegan) and has recurrent angular cheilosis, we prioritize testing for B12 and iron and discuss evidence‑based supplementation strategies.
Swollen, Red, Or Glossy Lips: Inflammation, Niacin Deficiency, Or Allergic Triggers
Lips that are unusually swollen, intensely red, or have a glossy, shiny surface often reflect an inflammatory process. Nutrition‑related causes include niacin deficiency (pellagra), while non‑nutritional causes like allergic contact dermatitis, angioedema, or infections are also common.
Niacin (vitamin B3) and mucocutaneous inflammation: Severe niacin deficiency leads to the classic triad of dermatitis, diarrhea, and dementia: mucosal redness and glossitis can be part of that syndrome. While pellagra is rare in developed countries, localized niacin deficiency or poor overall B‑vitamin status might contribute to lip inflammation in vulnerable populations.
Allergic and inflammatory causes: Cosmetics, dental products, flavored lip balms, and certain foods are frequent culprits. Angioedema can cause rapid lip swelling and may be triggered by medications (ACE inhibitors, NSAIDs), foods, or insect stings. Immunologic nutrient factors, low zinc or vitamin D, can worsen inflammatory responses, though they are rarely the singular cause of acute swelling.
What we do: If the swelling is acute and accompanied by breathing difficulty, we treat as an emergency and seek urgent care. For chronic or recurrent swelling, perform an allergy and medication history and trial removing suspected triggers for two to four weeks. Consider testing zinc levels and assessing overall diet quality: correcting low zinc (through meat, shellfish, legumes, or supplementation) supports mucosal immune defense. Topical calamine, cold compresses, and short courses of antihistamines or topical steroids (under guidance) can reduce symptoms while we identify underlying causes.
Frequent Cold Sores Or Slow Healing: Zinc And Immune‑Supporting Nutrients
Recurrent cold sores (herpes labialis) or lips that heal slowly often point to an immune system that’s not firing at full strength. Nutrition influences immune resilience, and zinc, vitamin C, vitamin D, and adequate protein intake are especially relevant for mucosal defense and wound healing.
Zinc’s role: Zinc is critical for immune cell function, epithelial repair, and antiviral defenses. Low zinc status is associated with delayed wound healing and increased susceptibility to infections. In practice, we see slower closure of fissures and recurrent herpes eruptions in people with inadequate zinc intake or malabsorption.
Other supportive nutrients: Vitamin C supports collagen synthesis and immune response, vitamin D modulates innate immunity and antiviral pathways, and adequate protein supplies amino acids for tissue repair. A deficiency in any of these can contribute to recurrent lesions or protracted healing.
Actionable steps: For frequent cold sores, consider daily lifestyle and nutrition measures, ensure dietary zinc (oysters, beef, chickpeas, pumpkin seeds), vitamin C (citrus, strawberries, bell peppers), and maintain adequate protein. Topically and pharmaceutically, we use antiviral agents (acyclovir, valacyclovir) for outbreaks and sometimes prophylaxis for frequent recurrences. If healing is unusually slow, request zinc and vitamin D testing along with a basic metabolic panel to rule out diabetes or other systemic contributors.
When supplementation helps: Short‑term zinc supplementation (10–25 mg/day) can improve healing in deficient individuals, but long‑term high doses require monitoring because excess zinc interferes with copper absorption. Coordinate supplementation with a clinician and use food first when possible.
Burning, Tingling, Or Numb Lips: B‑Vitamin Neuropathy And Other Nutritional Causes
Sensory disturbances of the lips, burning, tingling (paresthesia), or numbness, suggest neural involvement. Nutrient deficiencies that commonly affect peripheral nerves include B12, folate, and B6 (both deficiency and overdose can cause neuropathy). Other metabolic contributors like uncontrolled diabetes, alcohol use, or certain medications can produce similar symptoms.
B‑vitamin neuropathies: Vitamin B12 deficiency can produce sensory changes, often accompanied by other neurological signs (gait disturbance, paresthesias in hands/feet). Pyridoxine (B6) deficiency can cause neuropathic symptoms, yet paradoxically, very high doses of B6 can also cause sensory neuropathy. Folate deficiency typically presents with hematologic signs but can contribute to neurological symptoms when severe.
Differential diagnosis: Glossodynia (burning mouth syndrome) can be idiopathic or related to local oral conditions, dental factors, or systemic issues like xerostomia. Allergic reactions and autoimmune conditions (e.g., Sjögren’s) also deserve consideration.
Next steps: If lip burning or numbness is new, persistent, or progressive, investigate B12 and folate levels and review medication use (metformin, certain anticonvulsants, and proton pump inhibitors can impair B12). Check fasting glucose/HbA1c to screen for diabetes. For symptomatic relief, topical anesthetic gels or low‑dose tricyclics and gabapentin can help under clinical supervision while the underlying cause is treated.
Prevention and nutrition: For those at risk (older adults, strict vegetarians, people on long‑term acid suppression), routine B12 monitoring and appropriate oral or injectable supplementation prevents neuropathic complications before they become irreversible.
Darkening Or Hyperpigmentation Of The Lips: When To Consider Nutrient Causes Versus Other Conditions
Lip darkening or hyperpigmentation is usually benign and multifactorial. Causes range from sun exposure, smoking, and hormonal changes to post‑inflammatory hyperpigmentation and some medications. Nutrient causes are less common but worth considering in the right clinical context.
Nutritional considerations: Iron deficiency has been linked to mucocutaneous pallor rather than hyperpigmentation, but chronic cortisol or steroid imbalances (which can be related to malnutrition or chronic stress) might influence melanogenesis indirectly. Deficiencies in certain trace elements (e.g., copper) can influence pigmentation, though clear, direct links specific to lip hyperpigmentation are limited. Nutrient excess (high levels of phenolic compounds from certain foods or supplements) can sometimes cause discoloration.
Assessment strategy: Take a history focused on onset, progression, sun exposure, tobacco use, new medications (including herbal supplements), and ethnic baseline pigmentation variations. Look for associated mucosal changes (oral mucosa, tongue) and systemic symptoms. If pigmentation is isolated, stable, and without worrying features, we often observe and protect lips from sun exposure using SPF balms.
When to test or refer: Rapidly progressive darkening, asymmetry, ulceration, or a new pigmented lesion that changes warrants dermatology evaluation to rule out melanoma or other pathology. If nutritional deficiencies are suspected because of other signs (fatigue, hair loss, brittle nails), screen accordingly (CBC, ferritin, zinc, copper) and treat deficiencies as part of a broader plan.
Practical advice: Use broad‑spectrum sun protection on the lips, avoid tobacco, and review medications with your clinician. Most hyperpigmentation responds to addressing external contributors and cautious cosmetic approaches: true nutrient-driven pigmentation is rare but treatable when present.